
Introduction
A multitude of therapeutic approaches have historically been applied to the treatment of people with alcohol or
drug dependency. This article will include an overview of treatment models, while considering current best practice guidelines derived from professional literature and academic research. A critical analysis of evidence-based practice
will then be undertaken, while considering the implications for treatment within the New Zealand context.
Different Models of Addiction Treatment
The two philosophical stances underpinning treatment are the disease and harm reduction models, which each have divergent views on the nature of addiction (Denning, 2004). The ‘disease model’ views alcoholism as a lifelong illness that requires complete abstinence (Washton & Zweben, 2006), and is evident in 12-step programmes such as Alcoholics Anonymous (A.A) or Narcotics Anonymous (N.A). Interventions based on this model are based on the belief that clients “must be…persuaded to abstain from alcohol for the remainder of their lives” (Hester & Miller, 2003, p.4).
Therapeutic or support groups are often considered crucial to the integrated treatment of individuals with alcohol and drug problems (Connors, Donovan, & DiClemente, 2001; Kaufman, 1994). One benefit of 12-step groups is that they enhance social support, and provide strategies for coping with dependence, while promoting spiritual development. Due to difficulties in ensuring rigorous research, only a small number of randomised controlled trials have compared such groups with and other treatment approaches (Emmelkamp & Vedel, 2006). Some rehabilitation centres (e.g. Higher Ground, 2010) do however incorporate a 12-step philosophy into intensive treatment that includes group work, assessments, and individual counselling and case management.
In contrast to the disease model the harm reduction model espouses the belief that people with previous alcohol problems can maintain minimal substance use and drink/drug socially in a controlled manner (Valliant, 1996, cited Emmenkamp & Vedel, 2006). Such views are based on the premise that although abstinence is necessary in some cases, addiction is treatable. Harm reduction also relates to reducing risky behaviours associated with use and is epitomised by needle exchange programmes (ADIO, 2010) and the Community Alcohol and Drug Service methadone programme (CADS, 2010).
Phases of Addiction Treatment
The phases of treatment within alcohol and drug focused therapy consist of: 1) Assessment, 2) Goal setting and treatment planning, 3) Taking action and 4) Preventing relapse (Washton & Zweben, 2006). The widely endorsed biopsychosocial approach to assessment is widely used as it acknowledges the multifaceted influences that contribute towards addiction (Degler, 1991; Miller, 1985; Thombs, 1994; cited in Denning, 2004). Assessment often includes gathering historical information, observing patterns of substance use and assessing the level of risk or dependency (Glidden-Tracey, 2005; Washton & Zweben, 2006). Assessment sessions can also serve as an opportunity to implement “brief intervention” strategies such as advice on responsible levels of use (NZGG, 2008, pp.19-20). Once the assessment stage has been completed two key treatment plan factors are for the client to stop or curtail substance use, and to ameliorate the psychological and emotional problems causing or resulting from use (Gerald, 1992).
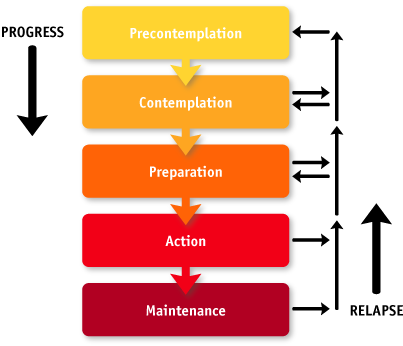
The New Zealand Guidelines Group states that a health practitioner’s task with regards to assessment and treatment is to “identify the patient’s current state of readiness to change and act appropriately” (NZGG, 2008, pp.19-21). Assessment tools such as the ‘stages of change readiness and treatment eagerness scale’ (SOC-RATES; Miller & Tonigan, 1996, cited in Connors et al, 2001) and the ‘Stages of Change’ or trans-theoretical model devised by Prochaska and DiClemente (1986) may therefore be useful. This model outlines the stages people go through when changing addictive behaviours. It also provides a framework to consider the most suitable interventions for clients who are in the pre-contemplation, contemplation, preparation, action, or maintenance stages (Connors et al, 2001).
Changes in Treatment Approaches and Attitudes Over Time
Approaches to working with alcohol and drug abusing clients have changed drastically over the last thirty years. Until the 1980’s the usual way of treating unmotivated or ambivalent clients was through confrontational methods, which included the intentional coordination of a crisis (Bratter, 1975, cited in Glidden-Tracey, 2005; Johnson, 1973, 1986, cited in Morgan & Litzke, 2008). Such approaches are not common today as they relate to high drop out rates and poor outcomes (Miller & Rollnick, 2002). This is verified by Stanton (2004, p.170), who found that success rates for confrontational interventions ranged from 0-36%, with the average being only 20%. Family interventions do not however have to involve confrontational interventions and couple or family treatments that consider the context of social systems have shown to be efficacious (Connors et al, 2001), and may also reduce attrition (Carrol & Oskin, 2005).
In line with recent evidence, researchers have advised alcohol and drug clinicians to adopt “a non-confrontational approach” (Hilarski, 2005, p.2), such as Motivational Interviewing (MI; Miller & Rollnick, 2002), which was found to be more effective in addressing alcohol abuse than confrontational counselling (Miller, Benefield & Tonigan, 1993). This widely sanctioned treatment approach integrates an empathic client-centred counselling style (e.g. Rogers, 1951) with more directive strategies in order to increase motivation and facilitate change among clients who may be ambivalent about reducing or stopping their substance use (Glidden-Tracey, 2005; Washton & Zweben, 2006).
Motivational Interviewing
Miller & Rollnick (1991, pp.20-28) explain that the “building blocks” of MI include ‘rolling with resistance’, giving feedback, removing barriers, providing choices, practicing empathy, clarifying goals and actively helping. Developing discrepancy and eliciting change talk are also important. Other principles include being positive and reassuring, avoiding pressuring tactics and supporting self-efficacy (Miller & Rollnick, 2002; Washton & Zweben, 2006).
 Several comprehensive studies or meta-analyses have proved the efficacy of MI (Miller, Benefield & Tonigan, 1993; Project MATCH, 1997; Stephens, Roffman & Curtin, 2000) and indicated strong empirical support for its use in improving client participation in treatment and reducing alcohol or drug use (Burke, Arkowitz & Menchola, 2003; Noonan & Moyers, 1997). Based on a systematic review of findings from 29 randomized controlled trials Dunn, DeRoo and Rivera (2001) also found that the strongest effects of MI were with problem drinkers (cited in Miller & Rollnick, 2002).
Several comprehensive studies or meta-analyses have proved the efficacy of MI (Miller, Benefield & Tonigan, 1993; Project MATCH, 1997; Stephens, Roffman & Curtin, 2000) and indicated strong empirical support for its use in improving client participation in treatment and reducing alcohol or drug use (Burke, Arkowitz & Menchola, 2003; Noonan & Moyers, 1997). Based on a systematic review of findings from 29 randomized controlled trials Dunn, DeRoo and Rivera (2001) also found that the strongest effects of MI were with problem drinkers (cited in Miller & Rollnick, 2002).
With regards to its use in treating drug dependency one meta-analysis (Saunders, Wilkinson & Phillips, 1995) discovered that MI was a useful adjunct to methadone treatment for opiate abusers and numerous randomised controlled trials demonstrated the feasibility of MI for other drug dependent populations including cannabis, cocaine and polydrug users (Dennis et al 2004, cited in Emmelkamp & Vedel, 2006, p.87).
While outcome studies of MI have overall had very positive results there is some uncertainty about what contributes to its success (Hilarski, 2005). There are also questions about large variations in outcome results as in some studies there was no significant effect at all (e.g. Hettema, Steel & Miller, 2005). One explanation could include the clinician’s level of training and skills, which may vary across therapists and treatment centres. Additionally, among some client groups MI has not proved to be as effective. Dual diagnosis clients for example do not seem to have the same positive results (Donovan, Rosengren, Downey, Cox & Sloan, 2001). This is problematic as a vast proportion of clients seeking treatment for alcohol or drug use also have mental health issues. With such clients CBT was also found to be superior to MI and 12-step approaches (Fisher & Bently, 1996; Jerrell & Ridgely, 1995).
Psychoanalytic / Psychodynamic Approaches
 Compared to other treatment methods psychoanalytic or psychodynamic therapies have received strong criticism and some authors claim there is no evidence verifying the efficacy of these approaches for treating alcohol and drug problems (Gerald, 1992; Rotgers et al, 2003). Furthermore, many underlying assumptions and techniques inherent in these approaches contradict “some basic principles that inform and guide the treatment of substance abuse” (Washton & Zweben, 2006, p.6). For example, delving into early (often traumatic) experiences and bringing unconscious material to the surface is likely to drive a client into heavier substance use as a way of coping with feelings that are overwhelming (Bender & Messner, 2003).
Compared to other treatment methods psychoanalytic or psychodynamic therapies have received strong criticism and some authors claim there is no evidence verifying the efficacy of these approaches for treating alcohol and drug problems (Gerald, 1992; Rotgers et al, 2003). Furthermore, many underlying assumptions and techniques inherent in these approaches contradict “some basic principles that inform and guide the treatment of substance abuse” (Washton & Zweben, 2006, p.6). For example, delving into early (often traumatic) experiences and bringing unconscious material to the surface is likely to drive a client into heavier substance use as a way of coping with feelings that are overwhelming (Bender & Messner, 2003).
Despite this caution, issues of a psychodynamic nature do arise in alcohol and drug therapy including developmental and attachment issues, defences, strong transference and counter-transference, and repetition of maladaptive patterns related to past experiences (Kaufman, 1994; Washton & Zweben, 2006). Such deep exploratory work may not however be possible until the client has successfully controlled substance use and increased ego strength. Contemporary psychodynamic psychotherapy approaches that incorporate attachment theory (Bowlby, 1982), revised Object Relations (Cashdan, 1988; Glickauf-Hughes & Wells, 1997), Relational Psychoanalytic (Mitchell, 1988, Mitchell & Aron, 1999), or Self Psychology (Kohut, 1996, 2001; Wolf, 1988) methodologies are however becoming increasingly accepted (Rotgers et al, 2003, p.3, Flores, 2004, p.3).
Cognitive Behavioural Therapies for Addiction
Cognitive and Behavioural approaches are also widely used with alcohol and drug using clients. In a meta-analysis of 17 studies Walters (2000) found that behavioural self control programs (training in drinking rate control, goal setting, identifying high risk situations, alternatives to alcohol use etc) were more effective than no treatment and at least as effective as abstinence based programs…at follow ups of one year or longer” (p.109). Carroll & Osken (2005) also noted that “contingency management, in which patients receive incentives or rewards for meeting specific behavioural goals has particularly strong, consistent and robust empirical support across a range of types of drug use” (p.1453).
 While contingency management showed greater immediate results, patients who had received CBT had better outcomes after a one-year follow up. Several other studies have shown that CBT has “strong empirical support for use in treatment of alcohol use disorders and have been demonstrated to be effective in drug taking populations as well” (Carroll & Osken, 2005, p.1454). It may not however be feasible for all alcohol and drug clinicians to receive adequate training in order to utilise CBT with the level of expertise that would ensure results concomitant with the research findings.
While contingency management showed greater immediate results, patients who had received CBT had better outcomes after a one-year follow up. Several other studies have shown that CBT has “strong empirical support for use in treatment of alcohol use disorders and have been demonstrated to be effective in drug taking populations as well” (Carroll & Osken, 2005, p.1454). It may not however be feasible for all alcohol and drug clinicians to receive adequate training in order to utilise CBT with the level of expertise that would ensure results concomitant with the research findings.
Awareness by clinicians of medication for addiction treatment also seems important (Rotgers et al, 2003; Volpicelli, Pettinati, McLellan, & O’Brien, 2001). One such medication is Naltrexone, which is widely used alongside talking therapies as a means of suppressing alcohol cravings. Many studies found that clients who were randomly assigned to Naltrexone had significantly fewer relapses than those in the placebo groups (eg. O’Malley et al, 1996; Rohsenow et al, 2000). From my own clinical experience I have found this medication to be useful in assisting my clients meet their goals of minimal use or abstinence. The problem with such pharmacological treatments however is compliance, as some clients may stop taking the medication if they intend to drink.
An Integrated Approach to Addiction Treatment
An integrated approach to working with clients is recommended that considers multiple contributing factors including emotional, biological, behavioural, cognitive, and social dimensions (Glidden-Tracey, 2005). Some authors also suggest integrating various therapeutic approaches. Kaufman (1994) and Galanter (1993) for example suggest CBT and MI at earlier stages followed by long-term psychodynamic work once sobriety is stabilized (cited in Rotgers et al, 2003, p.89). Washton & Zweben (2006) also describe how they draw on MI, CBT and Psychodynamic approaches.
Such ‘theoretical integrationism’ could make psychodynamic approaches more applicable for alcohol and drug treatment within the New Zealand health system. These syncretistic approaches seek to overcome the inadequacies and partiality of single theories through combining treatment methods from multiple modalities into a new coherent system (Norcross, 2005). From my own practice this is proved to be useful and allows me to integrate my personal approach with the requirements of the agencies where I have worked.
Research Findings: Evidence Based Practice?
The research backing such combined approaches includes McKee et al (2007, cited NZGG, 2008) who compared CBT with CBT enhanced by an initial session of MI for cocaine using clients. Although both treatments had similar results, clients who received the MI session in addition to CBT had higher motivation to change and “were more engaged”, attended more sessions during treatment and “reported more hope for abstinence and expected success” (NZGG, 2008, p.19). Another study found that while treatment results between CBT and MI were similar, clients receiving MI achieved similar results but in fewer sessions than those having CBT alone (Burke, Arkowitz & Menchola, 2003, p.857).
In order to evaluate treatment approaches Miller, Wilbourne, and Hetema (2003, cited in Hester & Miller, 2002) identified a total of 381 clinical trials and ranked the treatment approaches based on effectiveness and outcome. Top ranking treatments included brief intervention (1st), motivational enhancement (2nd) with other treatments including cognitive therapy (13th), 12-step facilitation (37th). Insight and exploratory psychotherapies accumulated one of the lowest scores of any of the treatment modalities.
One of the largest research studies designed to evaluate treatment approaches for alcohol abuse called Project MATCH (Matching Alcoholism Treatments to Client Heterogeneity; Project Match research group, 1977, cited Connors et al, 2001). In this study the 12 step facilitation (TSF) approach was compared to Motivational Enhancement Therapy (MET) and CBT. Results showed that treatment by TSF was “more or less equally effective as motivational enhancement and CBT (Project MATCH research Group, 1997, 1998, cited in Connors et al, 2001, p.105). It was however found that 12-step approaches are less effective if clients who are angry or resistant (MATCH research group, 1998 cited in NZGG, 2008). On the other hand if the client’s family and friends support drinking TSF was better than CBT or MET (Longabaugh, Wiltz, Zweben, & Stout, 1998; Project Match research group, 1998).
With regards to the therapeutic approaches classed as ‘not evidence-based’ it could be argued that this labelling may not be due to ineffectiveness, but rather to a lack of empirical research. This lack may in turn derive from the difficulty in measuring gradual but long-lasting changes in a persons’ inner world, sense of self or emotions (which are the goals of less evidence based approaches such as the psychodynamic approach), compared to treatment approaches that are more short-term and behaviourally based and can therefore be more easily measured.
The Therapeutic Relationship is the Most Important Factor
 Despite research attempting to prove the superiority of certain therapeutic modalities, numerous meta-analyses (e.g. Hovrath & Symond, 1991; Martin, Garske & Davis, 2000) have shown that the therapist-client relationship and the therapist’s attitude towards their client are the most significant variables effecting treatment outcome, irrespective of the theoretical approach or treatment used. Such findings are consistent with evidence linking ‘working alliance’ to improved outcomes in general psychotherapy literature (Moyers, Miller & Hendrickson, 2005). Washton & Zweben (2006) add that while numerous approaches have been proposed for alcohol and drug treatment, underlying any of these methodologies are the principles of starting where the patient is, ‘doing what works’ and most importantly ‘doing no harm’.
Despite research attempting to prove the superiority of certain therapeutic modalities, numerous meta-analyses (e.g. Hovrath & Symond, 1991; Martin, Garske & Davis, 2000) have shown that the therapist-client relationship and the therapist’s attitude towards their client are the most significant variables effecting treatment outcome, irrespective of the theoretical approach or treatment used. Such findings are consistent with evidence linking ‘working alliance’ to improved outcomes in general psychotherapy literature (Moyers, Miller & Hendrickson, 2005). Washton & Zweben (2006) add that while numerous approaches have been proposed for alcohol and drug treatment, underlying any of these methodologies are the principles of starting where the patient is, ‘doing what works’ and most importantly ‘doing no harm’.
As has been shown, health professionals within the alcohol and drug sector are currently able to access a vast amount of literature and utilise research findings and best-practice guidelines to direct their work (Rotgers, Mortensen, Waters, 2003). Such informed therapeutic work is referred to as Evidence Based Practice (EBP), which emphasises the application of empirically based treatments within clinical settings while considering client values and clinical acumen (Chatterjee, Poddar & Ameen, 2005). One aim of EBP is to eradicate harmful treatment and increase the use of helpful methods.
The utilisation of such effective approaches is of particular importance for working with substance using clients, who are often ambivalent about treatment. Unfortunately however, evidence-based treatment practices are still not widely used by alcohol and drug clinicians who infrequently incorporate current research findings into their work practice (Fals-Stewart & Birchler, 2002; Foreman, Bovasso & Woody, 2001; McGovern, Fox, Xie & Drake, 2004, cited in Emmelkamp & Vedel, 2006).
Cultural Considerations for Therapy
Another consideration regarding Evidence-based treatment approaches for alcohol and drug issues is whether these approaches are culturally sensitive to Maori and Pacific Island clients. Just because certain modalities have been validated through international research trials does not necessarily mean that they will be effective in the distinctive multi-cultural environment of Aotearoa/New Zealand.
Mason Durie (1999) put forward a culturally sensitive approach to counselling and therapy that assumes mental and emotional health problems derive from or are exacerbated by an insecure sense of self and problematic interpersonal relations. With this in mind it seems imperative that Maori and Pacific peoples are offered alcohol and drug treatment that acknowledges their own ethnic and cultural understandings. This need has been addressed within CADS by means of Pacific (Tupu) and Maori (Te Atea Marino) services.
Conclusion
In conclusion it has been shown that understandings and approaches aimed at addressing addiction continue to advance over time. The complexities of working with clients with alcohol and drug problems means that generic counselling and therapy methods may not be effectual, or may need to be adapted to work with this client group. Consideration of the research regarding evidence based treatment of alcohol and drug issues has led me to consider how these finding will influence my own clinical practice as a therapist and drug and alcohol counsellor. I believe it is essential to tailor evidence-based treatment approaches to clients’ specific circumstances. I do however tend to agree with Glidden-Tracey (2005, p.6) who states that therapy can make an impact and assist clients with drug and alcohol problems insofar as the client may “actualise the potential for a meaningful human interaction to occur”.
About the Author:
Cian Kerrisk is a Psychotherapist with Interim Registration from the Psychotherapists Board of Aotearoa New Zealand (PBANZ). He is a Registered Competent Practitioner with the Addiction Practitioners Association of New Zealand (DAPAANZ), a Provisional Member of the New Zealand Association of Psychotherapists (NZAP) and a Full member of the New Zealand Association of Counsellors (NZAC). He works part time as a Clinician for a DHB funded Addiction and Mental Health service and for Government Family and Community Services projects, as well as managing a small Private Practice (Synthesis Therapy and Cousnelling) in Ponsonby and Grey Lynn, Auckland.
References:
ADIO Trust (2010). Auckland Drug Information Outreach: Harm Reduction in Action (Brochure). Auckland, New Zealand: ADIO Trust.
Ball, S. A., Bachrach, K., Carol, K., DeCarlo, J., Farentinos, C., Obert, J., Van Horn, D., et al. (2007). Site Matters: Multisite Randomized Trial of Motivational Enhancement Therapy in Community Drug Abuse Clinics. In Journal of Consulting and Clinical Psychology, 75 (4), pp. 556-567.
Bender, S. & Messner, E. (2003). Becoming a therapist: What do I say and why? New York, NY: Guilford Press.
Bowlby, J. (1982). Attachment (2nd Ed). New York, NY: Basic Books.
Burke, B. L., Arkowitz, H., & Menchola, M. (2003). The efficacy of Motivational Interviewing: A meta-analysis of controlled clinical trials. Journal of Consulting and Clinical Psychology, 71 (5), 843-61.
Carroll, K. M, & Onken, L. S. (2005). Behavioural Therapies for Drug Abuse. In American Journal of Psychiatry, 162, 1452-1460.
Cashdan, S. (1988). Object Relations Therapy: Using the Relationship. New York, NY: Norton & Company.
Chatterjee, U., Poddar, A., & Ameen, S. (2005). Evidence Based Psychotherapy. Mental Health Reviews, retrieved 10th April, 2010 from http://www.cebm.net/glossary.asp
Connors, G., Donovan, D., & DiClemente, C. (2001) Substance Abuse Treatment and the Stages of Change: Selecting and Planning Interventions. New York, NY: Guilford Press.
Denning, P. (2004). Practicing Harm Reduction Psychotherapy: An alternative approach to addictions. New York, NY: Guilford Press.
Donovan, D. M., Rosengren, D. B., Downey, L., Cox, G. B. & Sloan, K.L. (2001). Attrition prevention with individuals awaiting publicly funded drug treatment. Addiction, 96, 1149-1160.
Emmelkamp, P., & Vedel, E. (2006). Evidence-based treatment for alcohol and drug abuse: A Practitioner’s Guide to Theory, Methods, and Practice. New York, NY: Rotledge.
Fisher, M.S., & Bently, K.J. (1996). Two group therapy models for clients with a dual diagnosis of substance abuse and personality disorder. Psychiatric Services, 47 (11), 1244-50.
Flores, P. J. (2004). Addiction as an attachment disorder. New York: Jason Aronson.
Gerald, M. (1992). Working with alcoholics and drug abusers in private practice: A psychoanalytic – Chemical dependency model. In Psychology of Addictive Behaviours, 6 (1), pp. 5-13.
Gelso, C. & Carter, J. (1985). The Relationship in counselling and psychotherapy: Components, consequences and theoretical antecendents. In The Counselling Psychologist, 13 (2), 155-243.
Glickauf-Hughes, C. & Wells, M. (1997). Object Relations Psychotherapy: An individualized and interactive approach to diagnosis and treatment. Northvale, NY: Jason Aronson Inc
Glidden-Tracey, C. E. (2005). Counselling and Therapy with clients who abuse Alcohol and Other Drugs. New Jersey: Lawrence Erlbaum Associates.
Graham, A. & Glickauf-Hughes, C. (1992). Object relations and addiction: The role of “transmuting externalizations”. Journal of Contemporary Psychotherapy, 22 (1).
Hester, R. K., & Miller, W. R. (2002). Handbook of alcoholism treatment approaches: Effective Alternatives. Boston, MI: Allyn & Bacon.
Hilarski, C. (2005). Addiction assessment and treatment with adolescents, adults and families. Binghampton, NY: The Haworth Press.
Jerrell, J. M. & Ridgely, M.S. (1997). Dual diagnosis care for severe and persistent disorders: A Comparison of three methods. Behavioural Healthcare Tomorrow, 6 (3), 26-33.
Kaufman, E. (1994). Psychotherapy of Addicted Persons. New York, NY: Guilford Press.
Miller, W. R., Benefield, R. G., & Tonigan, J. S. (1993). Enhancing motivation for change in problem drinking: A controlled comparison of two therapist styles. Journal of Consulting and Clinical Psychology, 61, 455-461.
Miller, W.R. & Rollnick, S. (2002). Motivational Interviewing: Preparing People for Change (2nd Ed.) New York: The Guilford Press.
Mitchell, S. A. (1988). Relational concepts in psychoanalysis: An integration. Cambridge, MA: Harvard University Press.
Mitchell, S. A. & Aron, L.. (1999). Relational Psychoanalysis: The Emergence of a Tradition. Hillsdale, NY: The Analytic Press.
Morgan, O. J., & Litzke, C. H. (Eds.) (2008). Family Intervention in Substance Abuse: Current Best Practices. Binghampton, NY: Hawthorn Press.
Moyers, T., Miller, W., & Hendrickson, S. (2005). How Does Motivational Interviewing Work? Therapist Interpersonal Skill Predicts Client Involvement Within Motivational Interviewing Sessions. Journal of Counselling and Clinical Psychology, 73 (4), 590-598.
New Zealand Guidelines Group (NZGG) (2008). Talking Therapies: A brief review of recent literature on the evidence. Retrieved 05 April, 2010 from www.nzgg.org.nz/guidelines/0040/full-guideline.pdf
Norcross, J. C. (2005). A primer on psychotherapy integration. In J. C. Norcross & M. R. Goldfried (Eds.), Handbook of psychotherapy integration (2nd ed., pp. 3-23). New York, NY: Oxford University Press.
O’Malley, S. S., Jaffe, A. J., Chang, G., Schottenfeld, R.S., Meyer, R. E., & Rounsaville, B. (1992). Naltrexone and coping skills therapy for alcohol dependence. A controlled study. Archives of General Psychiatry, 49, 881-887.
Rogers, C. (1951). Client-centered therapy: Its current practice, implications and theory. London, England: Constable Press.
Rohsenow, D. J., Monti, P. M., Hutchinson. K. E., Swift, R. M., Colby, S. M., & Kaplan, G, B. (2000). Naltrexone’s effects on reactivity to alcohol cues among alcoholic men. Journal of Abnormal Psychology, 109, 738-742.
Rotgers, F., Mortgenstern, J. & Walters, S. (2003). Treating Substance Abuse: Theory & Technique (2nd Ed.). New York: Guilford Press.
Saunders, B., Wilkinson, C. & Phillips, M. (1995). The impact of brief motivational intervention with opiate users attending a methadone programme. Addiction, 90, 415-424.
Stanton, M. D. (2004). Getting reluctant substance abusers to engage in treatment / self help: A review of outcomes and clinical options. Journal of Marital and Family Therapy, 30, 165-182.
Washton, A. M. & Zweben, J. E. (2006). Treating Alcohol and Drug Problems in Psychotherapy Practice: Doing What Works. New York: Guilford Press.
Wolf, E.S. (1988). Treating the Self: Elements of Clinical Self Psychology. New York: The Guilford Press.
Volpicelli J. R, Pettinati H. M, McLellan A. T, & O'Brien, C. P. (2001). Combining medication and psychosocial treatments for addictions: The BRENDA approach. New York, NY: Guilford Press.